Just as opioids weren’t a cure all, ketamine isn’t a cure all. In 2019, s-ketamine was approved for treatment-resistant depression (FDA)…and a huge warning flag should have been flown. Ketamine had already been approved in 1970, but that was for its original use for humans: an anesthetic. And in its original form it has already been abused, mainly as a party drug, meaning that it was typically used in social gatherings.
Let’s assume the FDA got it right and that intranasal ketamine – s-ketamine – does work for treatment-resistant depression. This ketamine was approved to be used only “under the supervision of a health care provider in a certified doctor’s office or clinic” (FDA). One of the big criticisms of the approval was that regular people don’t have the time or money for the cure: spending up to four hours per appointment – and there will be several appointments – in a medical professional’s office for infusion and monitoring.
Since s-ketamine was approved for treatment-resistant depression and ketamine was already approved for, well, anything, prescribers put two and two together and came up with a cash cow: ketamine clinics. But not for the intranasal kind that’s highly regulated, but the regular kind…the anesthetic…are popping up all over.
And ketamine, not s-ketamine, just regular, old ketamine, is being prescribed off label for anxiety to tinnitus and everything you can think of between (ACCP).
Does ketamine even WORK? Maybe. The results for s-ketamine, the highly regulated intranasal form, haven’t been thoroughly proven, as a recent Stanford Medicine News report indicates: “Stanford Medicine researchers found that a patient’s belief that they had received ketamine, even if they didn’t, could improve their depression” (Stanford). And there’s no research at all to indicate that it works for all its being prescribed for off label…and that’s worrisome.
But don’t take my word for it. Just watch any documentary or read any information about how the US got into the opioid crisis we did. The optics are the same. A drug is available and can be widely prescribed. People will feel better while using it, and there’s money to be made. What could possibly go wrong?
What, indeed. For starters, ketamine is still considered a party drug, which means that young people are the ones usually misusing it. And, parties don’t usually have only one drug to choose from, so it’s being used in conjunction with other drugs, including that most deadly of drugs, alcohol. And it’s still an anesthetic, which means that it represses breathing. So if it’s taken with any other drug that slows breathing – benzos, opioids, alcohol, to name a few – the effect is worsened, to the possible point of death.
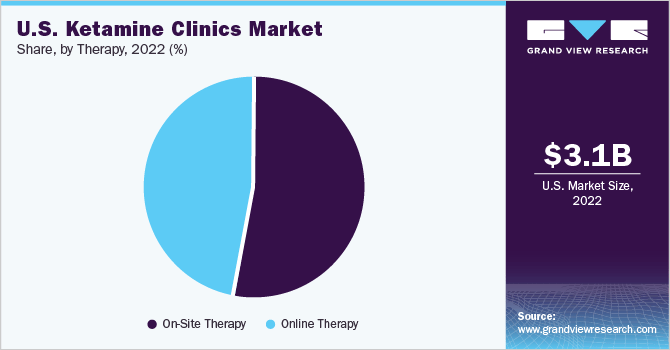
And the more prescriptions available, the more diversion that happens, and a lot of prescriptions are being written. Grand View Research indicates that “the U.S. ketamine clinics market size was valued at USD 3.1 billion in 2022 and is expected to grow at a compound annual growth rate (CAGR) of 10.63% from 2023 to 2030” (GrandViewResearch). Not bad for a new industry, huh?

This could seem like a reasonable response to a health crisis. But remember that the ketamine being prescribed is not the FDA-approved intranasal s-ketamine. It’s the anesthetic ketamine. Currently being prescribed for:
Anxiety
Bipolar Disorder
Chronic Pain
Depression
Eating disorders
Lyme disease
Major anxiety
Major depressive disorder
Migraines
Neuropathic pain syndrome
Obsessive-compulsive disorder
Pain
Peri-partum depression
Post-partum depression
PTSD
Restless leg syndrome
Rheumatoid arthritis
Substance use disorders
Tinnitus
Anything else a prescriber thinks it will work for…
And because it’s the anesthetic version of ketamine, there is no required monitoring in the clinician’s office. In fact, Grand View Research says that just under half of ketamine therapy is done online. So, yeah, not much monitoring going on there.
Ketamine is not a cure all, and neither will the next drug be. Full disclosure: daily, I take a mood-altering prescription, and my family and friends appreciate that. I’m not suggesting that no one should use prescriptions. I am, however, suggesting that we need to do our own research and be in charge of our own healthcare, because we should have learned SOMETHING from the opioid crisis, and that message certainly was not that we always get better living through pharmaceuticals.
References:
Click to access JCP-2021-Off%E2%80%90Label-Use-Ketamine-Challenging-Drug-Treatment.pdf
https://www.grandviewresearch.com/industry-analysis/us-ketamine-clinics-market-report
https://med.stanford.edu/news/all-news/2023/10/ketamine.html

Leave a comment